INTRODUCTION
In 2009, the Oxford Group reported a 1.8% rate of revision for pseudotumours in a series of 1419 hip resurfacings performed by multiple surgeons within a mean 4 year (0-9 years) time period and a 6% Kaplan-Meier failure rate for pseudotumour by 8 years. We were surprised by this high rate of failure due to a primary inflammatory reaction to metal bearings (pseudotumour) and we therefore wanted to evaluate our database for the incidence of failure we experienced due to pseudotumours.
METHODS
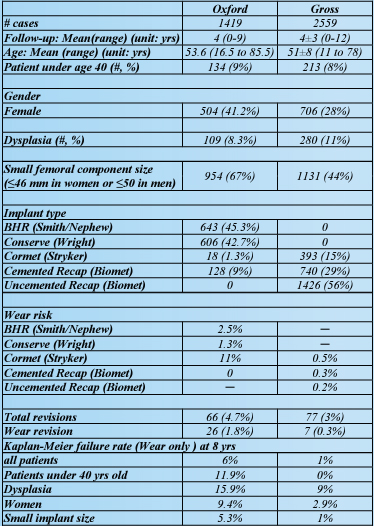
Between July 1999 and August 2011, a single surgeon performed 2559 metalon-metal hip resurfacing arthroplasties in 2109 patients. The mean length of follow-up was 4±3 years. We were able to achieve a follow-up rate of 92%. This study was compared to the multi-surgeon Oxford report on 1419 cases with 4 years follow-up. The Corin Cormet 2000 (393 cases) and Biomet Recap implants (2166 cases) were used in our series. All adverse wear failures had metal ion levels tested and had acetabular inclination angles measured on both supine and standing pelvis xrays. Similar to the Oxford Group, we analyzed wear related failures with “symptoms severe enough to cause revision”. A detailed comparison between the Oxford report and our database has been compiled (Table I).
RESULTS
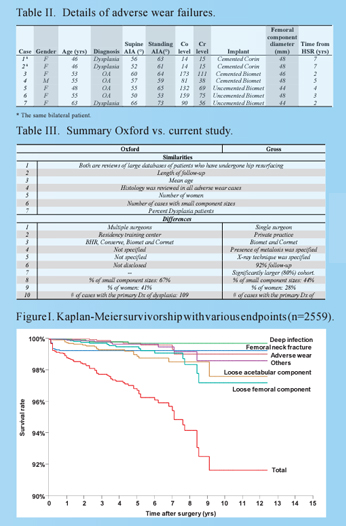
In this study, seven (0.27%) cases (six in female and one in male) out of 2559 cases were diagnosed as failures due to adverse wear with soft tissue and fluid accumulation, and metallosis seen at the time of surgery (Table II). The wear related failure rate was 0.27% (7/2559). Failures due to all other causes occurred in 70 (2.7%) cases. Revisions for adverse wear represented 9.1% of all failures. At 8 years post-operatively, our Kaplan-Meier cumulative revision rate for adverse wear was 1% for all patients (Fig I), 0.2% for men, 2.6% for Table I. Comparison between the Oxford study and the present study.
CONTINUED
women, and 9% for patients with a diagnosis of dysplasia. All adverse wear failures had component sizes ≤ 48 mm. All had metal ion levels of at least 15 ug/ml and acetabular inclination angles (AIA) >50° on standing pelvis radiographs. 5/7 had AIA > 60°. All had severe metallosis found at the time of revision. There were no failures from pseudotumours without evidence of adverse wear in this series (0/2559). In table III, we report the chief similarities and differences between the present study and the Oxford study.
CONCLUSIONS
In summary our data suggests the following conclusions: 1.) Adverse wear related failures (metallosis) are rare with the Biomet and Corin HRA systems (0.27%, Kaplan-Meier 1% at 10 years). 2.) Pseudotumours not related to adverse wear are rare with metal bearings. 3.) Adverse wear failures were seen with the Biomet and Corin systems only if the AIA on standing pelvis xray was > 50 degrees. (5/7 failures had AIA>60). 4.) A Safe zone for placing the Biomet and Corin devices is: AIA< 50 degrees on standing pelvis xrays. This likely also applies to other well-designed systems. 5.) Adverse wear failures are more common in women, dysplastics, and when femoral components ≤ 48 mm are required. These factors are, of course, interrelated. We therefore conclude that hip resurfacing with Biomet and Corin implants (and likely most others with a similar bearing design) is safe and effective and is exceedingly unlikely to result in adverse wear failure as long as the acetabular component is placed such that the AIA is < 50° on standing AP pelvis xray. In women with dysplasia that require small femoral components there is less room for error in acetabular component positioning. Adequately designed components exist; it is now up to surgeons to learn to place them accurately and reproducibly to avoid adverse wear failures.