
We perform multiple types of joint replacement including revision surgery and hip resurfacing arthroplasty. These are common procedures in hip surgery. We monitor all of our patient’s results long-term. The American population is highly mobile, and 80% of our patients come from outside of South Carolina. But we still maintain up-to-date follow-up in 96% of cases (many of our patients do not feel the need to follow up since they have excellent results with no pain; even if this is the case, we still recommend routine follow-up). We periodically update results for the most common procedures performed.
Survivorship Curves
We use the Kaplan-Meier method. This takes into account patients being lost to follow-up as well as deaths due to unrelated causes. Each failure is time-weighted by this method. The resulting curve provides the odds of an implant still being in place in the patient at any chosen time point from surgery. Joint replacements are not permanent. The longer that you follow a group of patients, the higher the failure rate that you record. It is very difficult to compare previous results to more recent cases because of the difference in follow-up. But if techniques improve, the survivorship curve of the latest group of patients will be higher and flatter than the previous group. The following results are some of the best in the world; see our publication section for a comparison of these results to other surgeons.
1. Hip Resurfacing
Hip Resurfacing Arthroplasty (HRA) is the best way to reconstruct a severely arthritic hip. It is more complicated to perform than a standard Total Hip Replacement (THR), therefore few surgeons are willing to offer this procedure. In the major joint registry reports, THR has better implant survivorship in most groups of patients, except in men with osteoarthritis who are under 60 years old. However, registries measure outcomes for average surgeons; The average surgeon performs less than 2.5 HRA cases/per year. This is not adequate to be an expert. In reports by high-volume hip resurfacing arthroplasty surgeons, results are much better than the registries suggest. We have now performed over 6700 Hip Resurfacing Arthroplasty (HRA) procedures over the last 20 years and currently perform nearly 500 cases/year.
The proven advantages of HRA are better function, longer implant survivorship, fewer dislocations, no thigh pain (from a THR stem), bone preservation, fewer wear/corrosion failures, and longer life expectancy than THR patients.
HRA does not result in a normal hip. But, when done by an expert, it more nearly approaches a normal hip in biomechanics and function, and patients are more likely to resume heavy work and impact sports than they could with a THR. Long-distance running is even possible for many (but not all) patients. Also, activities that require an extreme range of motion such as full squats, yoga, gymnastics, and ballet are possible because HRA has near-normal stability. Several other HRA surgeons in the world have reported similar long-term implant survivorship data. There is no large single surgeon report of THR that can match the results reported here at our practice.
Most failures occur during the first two years after surgery, which is why it is critical to severely limit activities in the first 6 months to allow adequate healing. After that, a patient can gradually return to completely unrestricted activity. There remains a slow rate of failure that occurs over time. But this does not seem to be affected by activity. Therefore, the overall failure rate increases for a group of patients as the length of follow-up increases. Herein, we report implant survivorship, for all three of our HRA implant groups (we no longer use Corin or Biomet hybrid implants; we exclusively use Biomet uncemented implants). Not all complications lead to failure. Below is a complete list of ALL major complications (not just failures/causes for revision) in the 5000 HRA cases using the Biomet uncemented system since 2007:
first
Your content goes here. Edit or remove this text inline or in the module Content settings. You can also style every aspect of this content in the module Design settings and even apply custom CSS to this text in the module Advanced settings.
FAILURES REQUIRING REVISION (up to 15-YEAR FOLLOW-UP)
- Femoral Neck Fracture
- Failure of Acetabular Ingrowth
- Adverse-Wear-Related Failure
- Femoral Head Collapse (Osteonecrosis)
- Late Acetabular Loosening
- Cup Shift
- Late Fracture
- Unknown Cause (revised elsewhere)
- Intertrochanteric Femoral Fracture
- Subluxation
- Unexplained Pain
- Femoral Head Fracture
- Subtrochanteric Femoral Fracture
- Impingement
- Recurrent Dislocation
- Deep Infection
TOTAL: 54 /5431 (1.0% of total cases)
COMPLICATIONS REQUIRING REOPERATION*
- Traumatic Intertrochanteric Fracture (5-11 months post-op)
- Deep Infection (cured)
- Hematoma
- Fascia Failure
- Superficial Infection (cured)
- Frostbite from an Ice Machine
- Suture Reaction
- Dislocation
- Abductor Tear
- Other/Misc
*Implants are not removed during reoperation.
TOTAL: 32/5431 (0.6% of total cases)
OTHER COMPLICATIONS*
- Acetabular Component Shift (nonsymptomatic)
- Cardiovascular Complication
- Dislocation
- Spinal Headache
- Urinary Complication
- Fracture
- Hematoma
- Other
- Peroneal Nerve Palsy
- Femoral Component Shift
- GI Bleed
- Loose Femoral Component
- Infection
- Femoral Notching
*No reoperation or revision required.
TOTAL: 106/5431 (2.0% of total cases)
RESURFACING SURVIVORSHIP
Includes ALL implant types*: 6700 cases over 20 years
*unless noted otherwise in each graph*
Survivorship of hip resurfacing continues to improve as we gain more experience and find measures to prevent failures. These survivorship curves allow the reader to see what the odds are that their implant will still be functioning at some point after implantation. We have used three implant systems in the last 20 years. Unless specified, the results include unselected consecutive patients (includes both genders, all ages, and all diagnoses). We present three Kaplan-Meier survivorship curves: all implant groups, all implants for patients under 50 at the time of surgery, and Biomet implants grouped by sex.
Unlike for THR, implant survivorship does not vary by age (overall 99.1-99.3% 13-year implant survivorship with the uncemented ReCap system in patients over 50 as well as those under 50 years). Men have slightly better 13-year implant survivorship (99.3%), but women are now only one percentage point lower (98.3%). If you look at only the most recent 10-year implant survivorship, women and men implant survivorship does not differ significantly (99.5% for men and 99.1% for women). Most failures occur in the first 1-2 years. If you make it to one year postoperative, your implant survivorship at 13 years is 99.6 %, If you make it to 2 years, this goes up to a 99.8% chance of implant survivorship at 13 years postoperative. Our uncemented resurfacing implant survivorship beats all registry benchmarks for THR regardless of age or sex.
A multicenter international study in which we participated recently was published in the journal Hip International. In 27 resurfacing centers in 13 countries over 11,000 cases in patients under age 50 with multiple different metal-on-metal resurfacing implant brands showed a 90% 20-year implant survivorship (93% in men and 81%in women). For comparison, total hip replacement registries show approximately 80% implant survivorship at 10 years and 50% at 20 years in this age group.
The Corin (pink) and Biomet hybrid (blue) are implants that we have used in the past. Notice that patient follow-up is longer for the Hybrid (cemented femoral) Biomet and the Corin groups. All Biomet hybrid implants (n=739) are now a minimum of 13 years old, and all Corin Hybrid implants (n=373) are at least 16 years old. Results are steadily improving with improvements in implants, knowledge about resurfacing, and surgeon experience. Current 13-year implant survivorship with the Biomet uncemented implants (n= 5431) is 99.1%. Limited 15-year data suggests survivorship remains at 99.1%.
Survivorship continues to improve with experience. The standard for “excellent survivorship” in Total Hip Replacement (THR) is >95% 10-year implant survivorship for patients of mean age 70. However, reported registry results for THR in patients under 50 are only 80% of 10-year implant survivorship. It can be seen here that the 10-year survivorship for our current implant, the uncemented (UC) Biomet ReCap, is at 99.1%. Implant survivorship does not drop off in our younger patients with HRA as it does for THR. THR lasts reasonably well in older folks for whom golf and walking are considered an “active” lifestyle, but they are not adequate for younger patients with a sporting lifestyle.
Women have historically had a higher implant failure rate with HRA than men. This is primarily due to two factors: Dysplasia is more common in women and carries a higher failure rate than any type of hip replacement. Also, women usually require smaller bearing sizes, which have been more prone to wear failure in HRA from edge loading resulting in metallosis. Both of these problems have been solved at our practice and are reflected in our improved results in women. The last wear failure was from a procedure performed in August 2009; the last acetabular failure due to dysplasia was from a procedure performed in December 2007. The latest 10-year implant survivorship calculation finds men and women are now equal at 99%, which is far better than the reported registry value of 80% 10-year survivorship for young men and women with THR.
The implant survivorship data reported here far surpasses joint implant registry data from Britain, Sweden, and Australia (for both THR and HRA) where these data types are kept. These are publicly available and you can access them online for free. Registry data can be thought of as average surgeon implant survivorship for purposes of a benchmark. But the most important factor in the outcome of any operation is individual surgeon skill. It is hard to know at which level a surgeon you are considering can perform. Anecdotal reports from a few patients or reputation are a poor substitute for data. Few surgeons provide written data such as we do.
Remember, implant survivorship is not the only factor that needs to be considered in deciding between THR and HRA. Other proven advantages of HRA are better functional outcomes, less residual thigh pain, fewer dislocations, bone preservation, and longer life expectancy.
After all revisions, reoperations, and complications are accounted for there are still approximately 2% of patients who experience moderate unexplained residual pain after HRA. The risk of moderate residual unexplained pain in THR is 20%. This means we cannot determine a specific reason why they are not satisfied. Some may have referred pain from their back or soft tissue problems we are unable to diagnose. In a THR, thigh pain from the stem is a common cause of residual pain. Residual pain may just represent the fact that HRA does not result in a normal hip. Because we can’t diagnose a cause, we don’t recommend revision surgery. If a revision is still performed, sometimes a patient improves, but most often they subject themselves to the risk of revision surgery and do not improve.
There is no measurable difference in the speed of recovery between THR and HRA.
We have included three distinct groups for your review. The first was the Corin Hybrid from 2001-2005, the next was the Biomet Hybrid from 2005-2007, and the final is the Biomet uncemented which we have used since 2007. You can see that results improve with each group. It is difficult to prove the exact reasons for the improvement. Some surgeons advocate patient selection to improve their results (perform total hips instead of resurfacing on higher-risk patients). Our goal is to allow all patients to realize the advantages of hip resurfacing. The rising survivorship curves in unselected patients prove that our philosophy works.
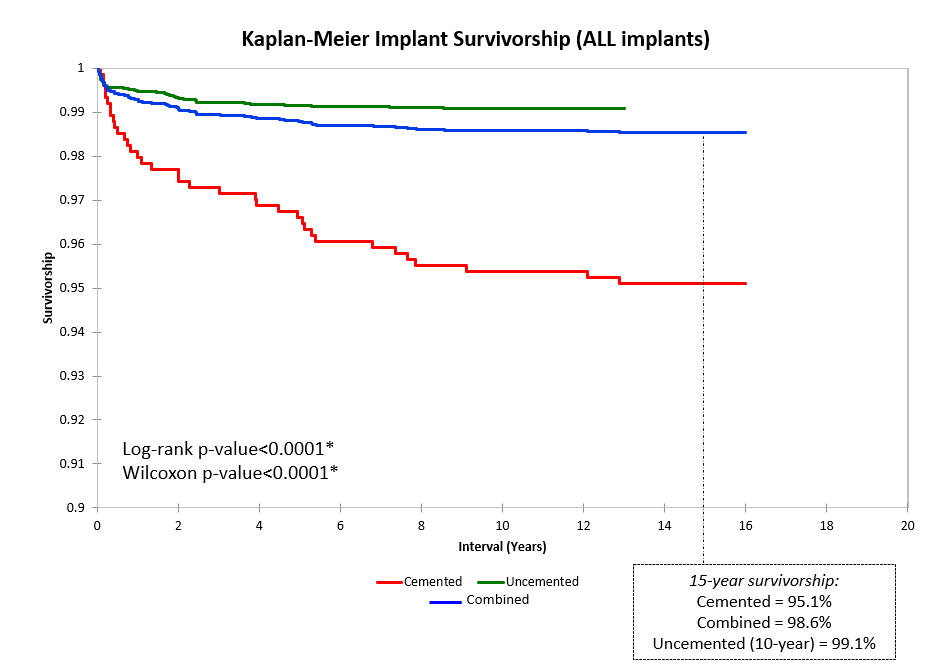
Survivorship curve for all three implants, as of 2022. All included cases have a minimum of 2 years of follow-up (surgeries performed in 2020 or earlier). Note that the survivorship y-axis begins at 80%. There have been no instances of adverse metal wear in cases after 2009.
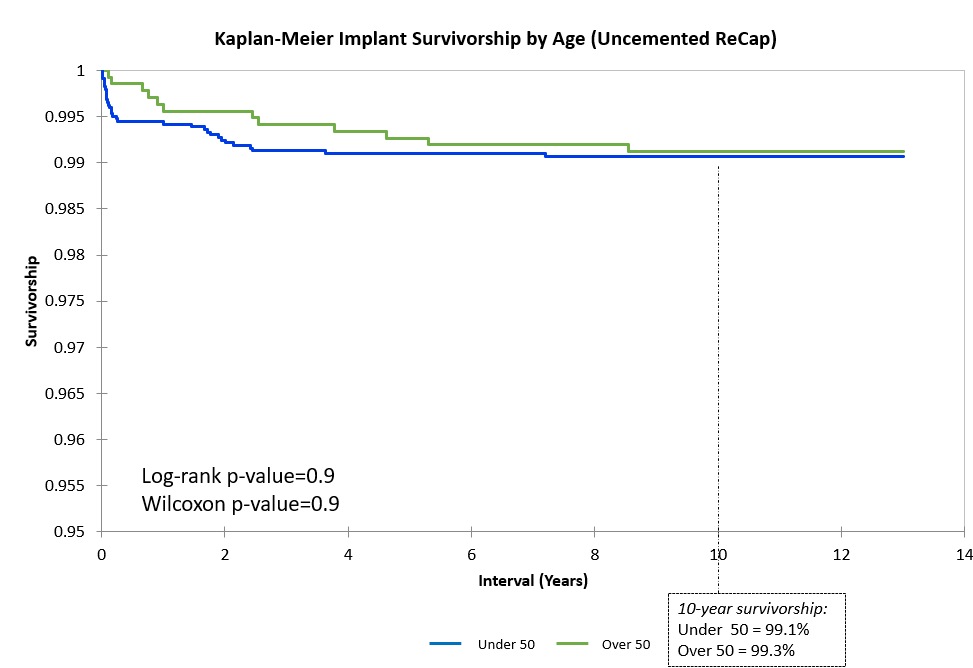
Above is the survivorship curve separated by age group for our uncemented ReCap group. Note the y-axis starts at 90%. There is no difference in survivorship or raw failure rate based on age. While many centers report greater rates of failure in younger patients, that is not the case at our practice. We pride ourselves on providing a durable arthroplasty option for young patients who wish to maintain their high levels of activity.
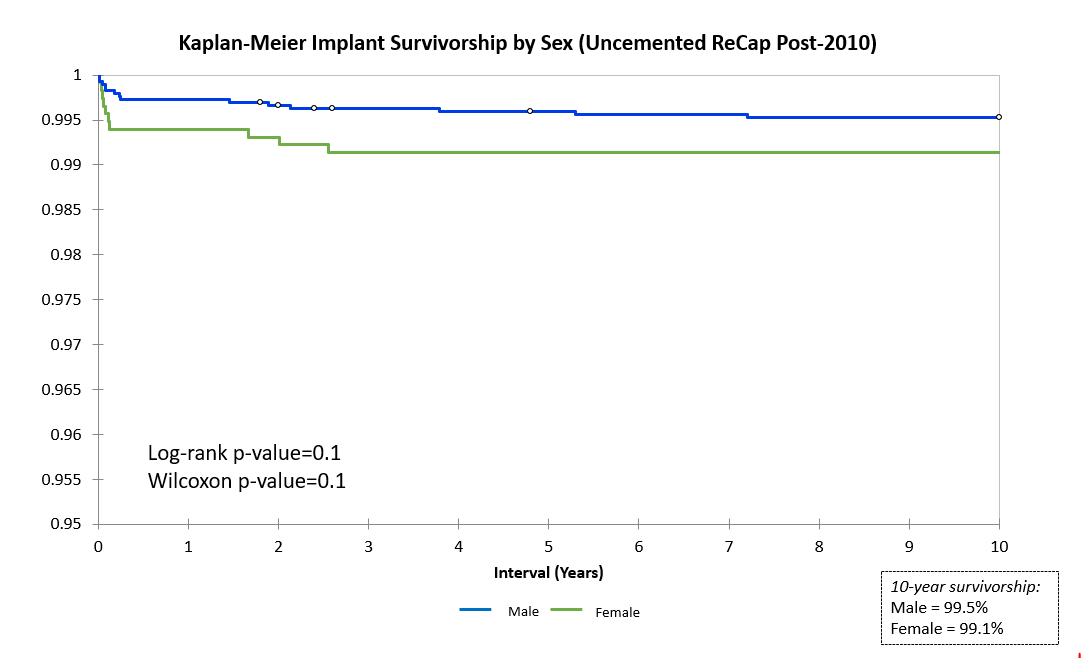
Many hip replacement surgeons exclude women from receiving surgery because of poor published results. We, however, elected to find out WHY implants in women were underperforming and to CORRECT implant design and surgical technique instead of excluding women from surgery. After the implementation of new protocols from 2007-2009, outcomes for women at our center have improved drastically (see our publication section ).
2. Total Hip Replacement
The need for a hip replacement continues to shrink as the complication rate for resurfacing falls. Hip resurfacing arthroplasty started as a temporary measure for younger patients to preserve bone. Most surgeons still prefer plastic-bearing hip replacement to hip resurfacing. Our first choice is usually hip resurfacing. In the few patients that are not good resurfacing candidates, our next choice used to be large metal bearing total hip replacement.
Hip dislocations are eliminated by this choice. Other surgeons are reluctant to use these implants because of a fear of adverse metal wear-related failure (AWRF). This has been a common failure mode among some brands (DePuy ASR recall 2010). But this is a rare problem with the Biomet design. Because of decreased demand for large metal bearing THR, Zimmer-Biomet discontinued the sale of this implant several years ago. We now use the best alternative which is a dual mobility ceramic/polyethylene bearing which is nearly as good.
With the large metal-bearing Biomet Magnum THR we have a 97% 15-year implant survivorship (for patients average age of 60) with no dislocations, which far surpasses registry benchmarks ( approximately 92% 10-year survivorship for a similar age group). Also, a standard total hip carries a 3% dislocation risk and a 1-5% trunion corrosion and requires permanent restrictions. We generally perform hip replacement in the very obese (BMI >35), patients older than 70 years, and those with severe osteoporosis, or severe bone deformities.
Failures in 211 cases with up to 16-year follow-up:
- Failure of Acetabular Ingrowth – 2
- Trunion Corrosion – 2
- AWRF due to Acetabular Malposition – 1
- Late Infection – 1
2.8% Raw Failure Rate (16 years postoperative)
3. Revision of Hip Resurfacing
Hip Resurfacing revision is more complicated than primary surgery. Our results are very close to those of our primary resurfacing cases with a 96% 8-year implant survivorship. Our most problematic group is revision for loose acetabular components. Other surgeons have had extremely poor results in revision for adverse wear-related failures (AWRF). Using an approach of limited debridement and repositioning of new metal-bearing acetabular components in more ideal inclination angles, we have had a 100% success rate in this problematic group.


