INTRODUCTION
A steep acetabular inclination angle is the primary cause of adverse wear related failure with well-designed metal-on-metal bearing hip resurfacing arthroplasties (HRA). One recent study demonstrated that positioning acetabular components of stemmed total hip arthroplasties (THA) within the “Lewinnek safe zone” is difficult; only 62% had AIA within the safe zone. However, we have previously demonstrated that acetabular components for HRA can be placed with an AIA<55° in 96% of cases using intraoperative X-ray. We now report our results using a refined technique, suggested by our previous study, as well as a lower acceptable limit for inclination angle (AIA<50°). We wanted to determine how often the method allowed us to achieve an AIA in the “safe zone for HRA”. We also wanted to know if repositioning an acetabular component intraoperatively to achieve an ideal position made it more likely to shift postoperatively.
METHODS
We evaluated radiographs of 513 consecutive metal-on-metal HRAs performed by a single surgeon between Oct 2010 and Mar 2012. Intra-operative, recovery room supine pelvis, first postoperative day standing pelvis, and 6-week standing pelvis X-rays were used to determine AIAs on all patients. Our previous study indicated that an intraoperative target inclination limit of 45° was required in order to have a final AIA<50° on postoperative supine pelvis XR 95% of the time. Therefore, in this series, if the intraoperative AIA was greater than 45°, the acetabular component was repositioned and another X-ray was taken to make sure it was within the target range. We prospectively recorded all cases in which a component was repositioned. The difference between the intra-operative AIA and the AIA on the standing postoperative day one X-ray were compared to evaluate the effectiveness of the intraoperative X-ray technique. In 144 of 513 HRA cases (28%) the acetabular component was repositioned during surgery. X-rays taken at 6 weeks were compared to the recovery room and postoperative day one X-rays to determine if any acetabular components shifted postoperatively.
Figure 1. Measurement of the acetabular inclination angle (α) is shown.
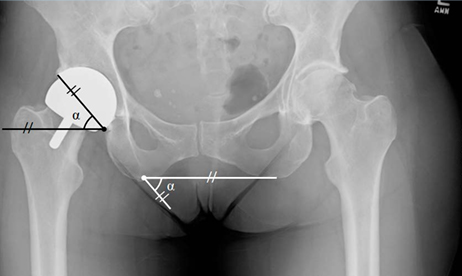
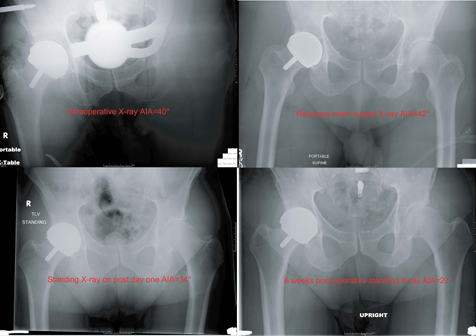
Figure 2. 67 years man with the primary diagnosis of OA and cam FAI. The acetabular component was not reposioned during the surgery, but shifted at 6 weeks post-operatively.
RESULTS
Only one of 513 cases had an AIA outside our “safe range for HRA” on the standing X-ray taken on the first postoperative day. In this case, the intraoperative radiograph showed an AIA of 40°, while it was 50° on the standing postoperative radiograph. The acetabular component was judged not to have shifted. In all of the remaining 512 (99.8%) cases the AIA was within the safe range of AIA< 50°. The average absolute difference between the AIA on the portable intra-operative X-rays and the AIA on the standing X-ray on post day one was 2.6°±2.9° (range: 0° to 26°). The variance was ≥ 5° in 83 (16.2%) cases and was ≥ 10° in 20 (3.9%) cases. One (0.7%) component in the group in which the acetabular component was repositioned during surgery was found to have shifted by the 6 week visit, while five (1.4%) components in the remaining 369 cases (without intraoperative repositioning) were found to have shifted (P=0.5).
CONCLUSIONS
In summary:
- In 99.8% (512/513) cases, an AIA<50° was achieved on post day one standing X-ray using an intraoperative target of AIA<45°.
- The difference of the measured AIA between the intraoperative and the postoperative standing pelvis XR was 2.6°±2.9°.
- 28% cups required intraoperative repositioning to achieve the intraoperative target.
- 1 % (6/513) acetabular components shifted postoperatively without adverse consequences.
- Repositioning acetabular components did not increase the chance of a postoperative cup shift.
Message: We suggest measuring an intraoperative AIA and repositioning the acetabular component until the AIA< 45°.
Table 1: Patient information of the study group.
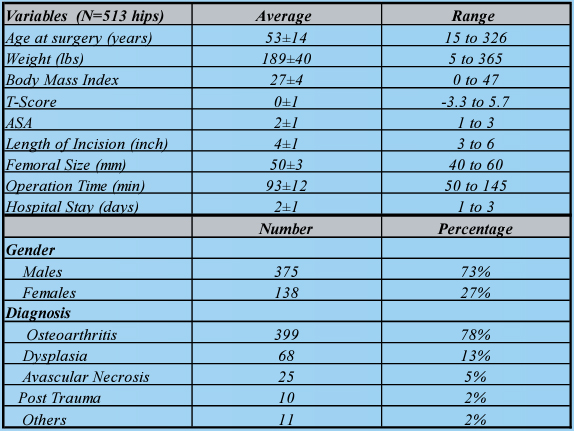
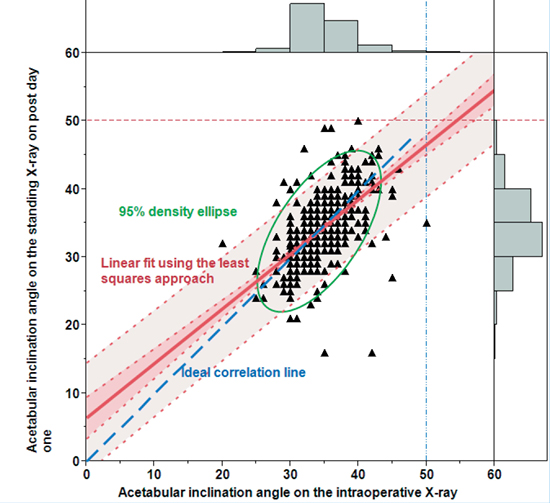
Figure 3. Comparison between AIA on the intra-operative X-ray and AIA on the standing X-ray on post day one suggests a high correlation between these two angles.